

The surgeon general tweeted: “STOP BUYING MASK, they are not effective…”. The Center for Disease Controls (CDC) states that surgical masks offer far less protection than the N95 respirator masks (which also must be perfectly fitted and only professionals can do it). The CDC recommends that healthy persons should not wear masks at all, only the sick ones. These guidelines are not rooted in scientific rationales but were motivated by the need to save the valuable masks for health professionals in view of a shortage. But they may have had unintended consequences: stigmatizing those that wear masks in the public (you are a hoarder, or you are contagious!)
Contrast this with the cultural habit, the encouragement, or even mandate to wear masks in Asian countries — which have now “flattened the curve” or even have had a flatter curve from the beginning.
Sure, surgical masks, and improperly worn N95 respirator masks, do not offer perfect protection. But if the stated goal is to “flatten” the curve (as opposed to eradication of the virus), we have to abandon the black-and-white thinking, and embrace shades of grey. We cannot any longer claim that masks “are not effective”. We cannot allow the perfect to be the enemy of the good. What if a however partial protection afforded by leaky surgical or even self-made masks reduces transmission probability to an extent that is similar to that of the recommended (equally imperfect) distancing by more than 6 feet from each other or “not touching your face”? It could then double the impact of non-pharmacological intervention (NPI) on flattening the curve (FIG. 1).
![]()
Since the CDC provides no scientific evidence for its statement that masks worn by the public “are not effective”, here we review the scientific support for protection conferred by surgical masks. We focus on mechanistic rationale (as opposed to epidemiological-phenomenological evidence). We conclude, by considering cough droplet ballistics and the latest research findings on the biology of transmission of the SARS-CoV2 virus (which causes COVID-19) that any physical barrier, as provided even by make-shift masks, may substantially reduce the spread of COVID 19. If we are soon to yield to the pressure to loosen lockdowns and allow limited social interactions to revive the economy, then public masks should have a role and could facilitate a middle-of-the-road approach.
The official recommendation by CDC, FDA and others that masks worn by the non-health-care professionals are ineffective is incorrect at three levels: In the logic, in the mechanics of transmission, and in the biology of viral entry.
I. THE LOGIC
Of course no mask, be it the tight-fitting NIOSH approved N95 respirator mask or the loosely worn surgical mask, provide perfect (“100%”) protection. But imperfect protection does not mean “completely useless”, much as a glass not full need not be empty: I would gladly accept a glass of water filled to 60 % when I am thirsty. Absence of evidence (of protection) is not evidence of absence. But in our binary world, the official message that surgical masks are “not effective” may have sent the wrong message: that they are absolutely useless. Sadly, with the black-and-white picture painted by officials, the discussion about the effectiveness of masks has been stifled, and with it the possibility of incentivizing industry to ramp up production of these 75 cents-a-piece protective devices.
But with the declared goal to “flatten the curve” (and not to totally eliminate the virus) we have a “relative” as opposed to absolute goal, which places the notion of “partial protection” in a new light. In principle, one could compute the extent Y of flattening of the curve given a partial protection by X % as conferred by mask. But for that we need to first understand the mechanics and biology of transmission in detail.
II. THE MECHANICS
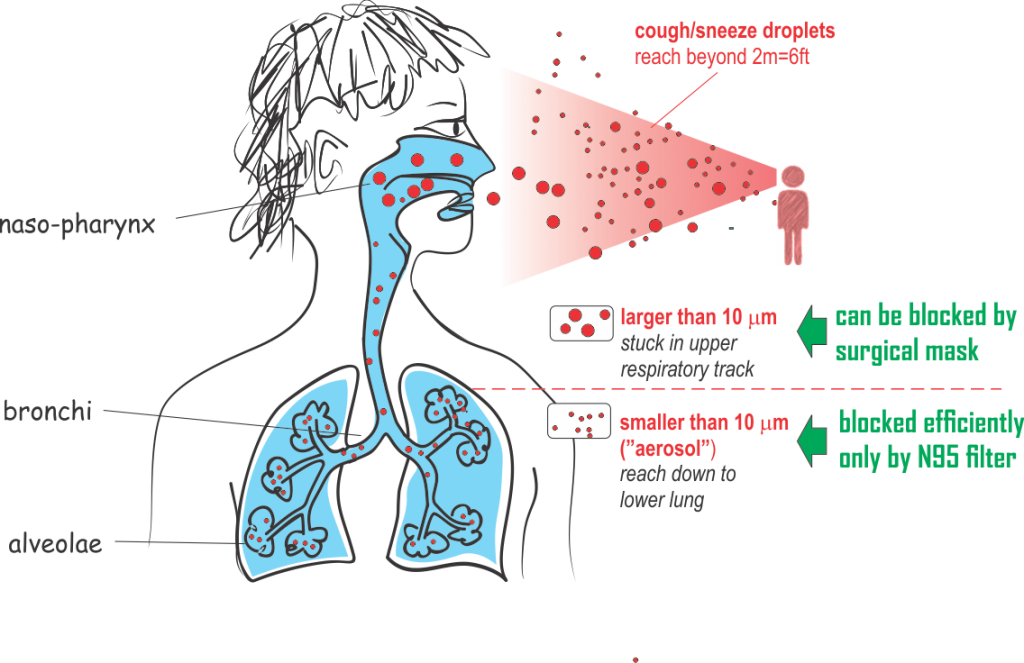
How viruses that cause airborne diseases are carried by droplets from person to person is a complicated, understudied matter. Droplets can (for this discussion) be crudely divided in two large categories based on size (FIG. 2):
![]()
(a) Droplets below a diameter of 10 um (micrometer), the upper size limit for the definition of ‘aerosol’ (particles so light as to be able to float in the air). For brevity, let us call this category “aerosols”. These small aerosols are carried by ventilation or by winds and thus can travel across rooms. What makes N95 facial masks different from the surgical masks is that the former are designed (as per regulatory requirement) to stop aerosols: they have to filter out 95% of droplets smaller than 0.3 um.
(b) Droplets larger than 10um (micrometer), reaching 100um or more. Let us call these large particles “spray droplets” here. (For a more detailed discussion, see Nicas and Jones, 2009). Of course, droplets can be even larger, up to a size visible to the naked eye in the spray generated by coughing or sneezing (0.1 um diameter to above). Calculations by Xie et al suggest that if exhaled, the >0.1 um droplets may evaporate or fall to a surface within 2m, depending on size, air humidity and temperature. But coughing or sneezing can shoot them like projectiles out of the mouth with a “muzzle velocity” of 50 meters/second (for sneezing) or 10 m/s (for coughing), and droplets can reach distances as far as 6m away. If so, then the much mentioned “safe distance” of 6 feet in social encounters may not suffice — except you wear a (simple) mask –more on that later.
Fuente y más información: www.medium.com
5,000 total views, 2 views today
0 Comments